Types of Brain Tumors
A brain tumor, known as an intracranial tumor, is an abnormal mass of tissue in which cells grow and multiply uncontrollably, seemingly unchecked by the mechanisms that control normal cells. More than 150 different brain tumors have been documented, but the two main groups of brain tumors are termed primary and metastatic.
Primary brain tumors include tumors that originate from the tissues of the brain or the brain’s immediate surroundings. Primary tumors are categorized as glial (composed of glial cells) or non-glial (developed on or in the structures of the brain, including nerves, blood vessels and glands) and benign or malignant.
Metastatic brain tumors include tumors that arise elsewhere in the body (such as the breast or lungs) and migrate to the brain, usually through the bloodstream. Metastatic tumors are considered cancer and are malignant.
Metastatic tumors to the brain affect nearly one in four patients with cancer, or an estimated 150,000 people a year. Up to 40 percent of people with lung cancer will develop metastatic brain tumors. In the past, the outcome for patients diagnosed with these tumors was very poor, with typical survival rates of just several weeks. More sophisticated diagnostic tools, in addition to innovative surgical and radiation approaches, have helped survival rates expand up to years; and also allowed for an improved quality of life for patients following diagnosis.
Types of Benign Brain Tumors
Chordomas are benign, slow-growing tumors that are most prevalent in people ages 50 to 60. Their most common locations are the base of the skull and the lower portion of the spine. Although these tumors are benign, they may invade the adjacent bone and put pressure on nearby neural tissue. These are rare tumors, contributing to only 0.2 percent of all primary brain tumors.
● Craniopharyngiomas typically are benign, but are difficult tumors to remove because of their location near critical structures deep in the brain. They usually arise from a portion of the pituitary gland (the structure that regulates many hormones in the body), so nearly all patients will require some hormone replacement therapy.
● Gangliocytomas, gangliomas and anaplastic gangliogliomas are rare tumors that include neoplastic nerve cells that are relatively well-differentiated, occurring primarily in young adults.
● Glomus jugulare tumors most frequently are benign and typically are located just under the skull base, at the top of the jugular vein. They are the most common form of glomus tumor. However, glomus tumors, in general, contribute to only 0.6 percent of neoplasms of the head and neck.
● Meningiomas are the most common benign intracranial tumors, comprising 10 to 15 percent of all brain neoplasms, although a very small percentage are malignant. These tumors originate from the meninges, the membrane-like structures that surround the brain and spinal cord.
● Pineocytomas are generally benign lesions that arise from the pineal cells, occurring predominantly in adults. They are most often well-defined, noninvasive, homogeneous and slow-growing.
● Pituitary adenomas are the most common intracranial tumors after gliomas, meningiomas and schwannomas. The large majority of pituitary adenomas are benign and fairly slow-growing. Even malignant pituitary tumors rarely spread to other parts of the body. Adenomas are by far the most common disease affecting the pituitary. They commonly affect people in their 30s or 40s, although they are diagnosed in children, as well. Most of these tumors can be treated successfully.
● Schwannomas are common benign brain tumors in adults. They arise along nerves, comprised of cells that normally provide the “electrical insulation” for the nerve cells. Schwannomas often displace the remainder of the normal nerve instead of invading it. Acoustic neuromas are the most common schwannoma, arising from the eighth cranial nerve, or vestibularcochlear nerve, which travels from the brain to the ear. Although these tumors are benign, they can cause serious complications and even death if they grow and exert pressure on nerves and eventually on the brain. Other locations include the spine and, more rarely, along nerves that go to the limbs.
Types of Malignant Brain Tumors
Gliomas are the most prevalent type of adult brain tumor, accounting for 78 percent of malignant brain tumors. They arise from the supporting cells of the brain, called the glia. These cells are subdivided into astrocytes, ependymal cells and oligodendroglial cells (or oligos). Glial tumors include the following:
● Astrocytomas are the most common glioma, accounting for about half of all primary brain and spinal cord tumors. Astrocytomas develop from star-shaped glial cells called astrocytes, part of the supportive tissue of the brain. They may occur in many parts of the brain, but most commonly in the cerebrum. People of all ages can develop astrocytomas, but they are more prevalent in adults — particularly middle-aged men. Astrocytomas in the base of the brain are more prevalent in children or younger people and account for the majority of children’s brain tumors. In children, most of these tumors are considered low-grade, while in adults, most are high-grade.
● Ependymomas are derived from a neoplastic transformation of the ependymal cells lining the ventricular system and account for two to three percent of all brain tumors. Most are well-defined, but some are not.
● Glioblastoma multiforme (GBM) is the most invasive type of glial tumor. These tumors tend to grow rapidly, spread to other tissue and have a poor prognosis. They may be composed of several different kinds of cells, such as astrocytes and oligodendrocytes. GBM is more common in people ages 50 to 70 and are more prevalent in men than women.
● Medulloblastomas usually arise in the cerebellum, most frequently in children. They are high-grade tumors, but they are usually responsive to radiation and chemotherapy.
● Oligodendrogliomas are derived from the cells that make myelin, which is the insulation for the wiring of the brain.
Other Types of Brain Tumors
● Hemangioblastomas are slow-growing tumors, commonly located in the cerebellum. They originate from blood vessels, can be large in size and often are accompanied by a cyst. These tumors are most common in people ages 40 to 60 and are more prevalent in men than women.
● Rhabdoid tumors are rare, highly aggressive tumors that tend to spread throughout the central nervous system. They often appear in multiple sites in the body, especially in the kidneys. They are more prevalent in young children, but also can occur in adults.
Pediatric Brain Tumors
Brain tumors in children typically come from different tissues than those affecting adults. Treatments that are fairly well-tolerated by the adult brain (such as radiation therapy) may prevent normal development of a child’s brain, especially in children younger than age five.
According to the Pediatric Brain Tumor Foundation, approximately 4,200 children are diagnosed with a brain tumor in the U.S. Seventy-two percent of children diagnosed with a brain tumor are younger than age 15. In some patients the descended cerebellar components are debulked or removed.
Some types of brain tumors are more common in children than in adults. The most common types of pediatric tumors are medulloblastomas, low-grade astrocytomas (pilocytic), ependymomas, craniopharyngiomas and brainstem gliomas.
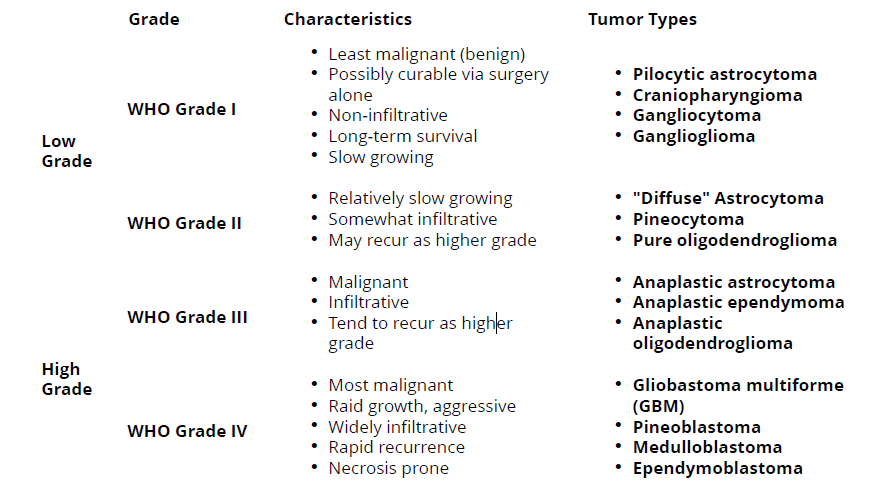
The World Health Organization (WHO) has developed a grading system to indicate a tumor’s malignancy or benignity based on its histological features under a microscope.
● Most malignant
● Rapid growth, aggressive
● Widely infiltrative
● Rapid recurrence
● Necrosis prone
World Health Organization (WHO) Brain Tumor Grades
Incidence in Adults
The National Cancer Institute estimates that 22,910 adults (12,630 men and 10,280 women) will be diagnosed with brain and other nervous system tumors in 2012. It also estimates that in 2012, 13,700 of these diagnoses will result in death. Between 2005 and 2009, the median age for death from cancer of the brain and other areas of the nervous system was age 64.
Brain Tumor Causes
Brain tumors are thought to arise when certain genes on the chromosomes of a cell are damaged and no longer function properly. These genes normally regulate the rate at which the cell divides (if it divides at all) and repair genes that fix defects of other genes, as well as genes that should cause the cell to self-destruct if the damage is beyond repair. In some cases, an individual may be born with partial defects in one or more of these genes. Environmental factors may then lead to further damage. In other cases, the environmental injury to the genes may be the only cause. It is not known why some people in an “environment” develop brain tumors, while others do not.
Once a cell is dividing rapidly and internal mechanisms to check its growth are damaged, the cell can eventually grow into a tumor. Another line of defense may be the body’s immune system, which optimally would detect the abnormal cell and kill it. Tumors may produce substances that block the immune system from recognizing the abnormal tumor cells and eventually overpower all internal and external deterrents to its growth.
A rapidly growing tumor may need more oxygen and nutrients than can be provided by the local blood supply intended for normal tissue. Tumors can produce substances called angiogenesis factors that promote the growth of blood vessels. The new vessels that grow increase the supply of nutrients to the tumor, and, eventually, the tumor becomes dependent on these new vessels. Research is being done in this area, but more extensive research is necessary to translate this knowledge into potential therapies.
Symptoms
Symptoms vary depending on the location of the brain tumor, but the following may accompany different types of brain tumors:
● Headaches that may be more severe in the morning or awaken the patient at night
● Seizures or convulsions
● Difficulty thinking, speaking or articulating
● Personality changes
● Weakness or paralysis in one part or one side of the body
● Loss of balance or dizziness
● Vision changes
● Hearing changes
● Facial numbness or tingling
● Nausea or vomiting, swallowing difficulties
Diagnosis
Sophisticated imaging techniques can pinpoint brain tumors. Diagnostic tools include computed tomography (CT or CAT scan) and magnetic resonance imaging (MRI). Other MRI sequences can help the surgeon plan the resection of the tumor based on the location of the normal nerve pathways of the brain. Intraoperative MRI also is used during surgery to guide tissue biopsies and tumor removal. Magnetic resonance spectroscopy (MRS) is used to examine the tumor’s chemical profile and determine the nature of the lesions seen on the MRI. Positron emission tomography (PET scan) can help detect recurring brain tumors.
Sometimes the only way to make a definitive diagnosis of a brain tumor is through a biopsy. The neurosurgeon performs the biopsy and the pathologist makes the final diagnosis, determining whether the tumor appears benign or malignant, and grading it accordingly.
Brain Tumor Treatment
Brain tumors (whether primary or metastatic, benign or malignant) usually are treated with surgery, radiation, and/or chemotherapy — alone or in various combinations. While it is true that radiation and chemotherapy are used more often for malignant, residual or recurrent tumors, decisions as to what treatment to use are made on a case-by-case basis and depend on a number of factors. There are risks and side effects associated with each type of therapy.
Surgery
It is generally accepted that complete or nearly complete surgical removal of a brain tumor is beneficial for a patient. The neurosurgeon’s challenge is to remove as much tumor as possible, without injuring brain tissue important to the patient’s neurological function (such as the ability to speak, walk, etc.). Traditionally, neurosurgeons open the skull through a craniotomy to insure they can access the tumor and remove as much of it as possible. A drain (EVD) may be left in the brain fluid cavities at the time of surgery to drain the normal brain fluid as the brain recovers from the surgery. Another procedure that is commonly performed, sometimes before a craniotomy, is called a stereotactic biopsy. This smaller operation allows doctors to obtain tissue in order to make an accurate diagnosis. Usually, a frame is attached to the patient’s head, a scan is obtained, and then the patient is taken to the operating area, where a small hole is drilled in the skull to allow access to the abnormal area. Based on the location of the lesion, some hospitals may do this same procedure without the use of a frame. A small sample is obtained for examination under the microscope.
In the early 1990s, computerized devices called surgical navigation systems were introduced. These systems assisted the neurosurgeon with guidance, localization and orientation for tumors. This information reduced the risks and improved the extent of tumor removal. In many cases, surgical navigation systems allowed previously inoperable tumors to be excised with acceptable risks. Some of these systems also can be used for biopsies without having to attach a frame to the skull. One limitation of these systems is that they utilize a scan (CT or MRI) obtained prior to surgery to guide the neurosurgeon. Thus, they cannot account for movements of the brain that may occur intraoperatively. Investigators are developing techniques using ultrasound and performing surgery in MRI scanners to help update the navigation system data during surgery.
Intraoperative language mapping is considered by some as a critically important technique for patients with tumors affecting language function, such as large, dominant-hemisphere gliomas. This procedure involves operating on a conscious patient and mapping the anatomy of their language function during the operation. The doctor then decides which portions of the tumor are safe to resect. Recent studies have determined that cortical language mapping may be used as a safe and efficient adjunct to optimize glioma resection while preserving essential language sites.
Ventriculoperitoneal shunting may be required for some patients with brain tumors. Everyone has cerebrospinal fluid (CSF) within the brain and spine that is slowly circulating all the time. If this flow becomes blocked, the sacs that contain the fluid (the ventricles) can become enlarged, creating increased pressure within the head, resulting in a condition called hydrocephalus. If left untreated, hydrocephalus can cause brain damage and even death. The neurosurgeon may decide to use a shunt to divert the spinal fluid away from the brain and, therefore, reduce the pressure. The body cavity in which the CSF is diverted usually is the peritoneal cavity (the area surrounding the abdominal organs). The shunt usually is permanent. If it becomes blocked, the symptoms are similar to that of
the original condition of hydrocephalus and may include headaches, vomiting, visual problems and/or confusion or lethargy, among others. Another method that may be used to control obstruction of the brain fluid pathways is called an Endoscopic Third Ventriculostomy. This helps the brain fluid be diverted around the obstruction without the need for a shunt.
Radiation Therapy
Radiation therapy uses high-energy X-rays to kill cancer cells and abnormal brain cells and to shrink tumors. Radiation therapy may be an option if the tumor cannot be treated effectively through surgery.
● Standard External Beam Radiotherapy uses a variety of radiation beams to create a conformal coverage of the tumor while limiting the dose to surrounding normal structures. The risk of long-term radiation injury with modern delivery methods is very low. Newer techniques of delivery aside from 3-dimensional conformal radiotherapy (3DCRT) include intensity-modulated radiotherapy (IMRT).
● Proton Beam Treatment employs a specific type of radiation in which protons, a form of radioactivity, are directed specifically to the tumor. The advantage is that less tissue surrounding the tumor incurs damage.
● Stereotactic Radiosurgery (such as Gamma Knife, Novalis and Cyberknife) is a technique that focuses the radiation with many different beams on the target tissue. This treatment tends to incur less damage to tissues adjacent to the tumor. Currently, there is no data to suggest one delivery system is superior to another in terms of clinical outcome, and each has its advantages and disadvantages.
Chemotherapy
Chemotherapy generally is considered to be effective for specific pediatric tumors, lymphomas and some oligodendrogliomas. While it has been proven that chemotherapy improves overall survival in patients with the most malignant primary brain tumors, it does so in only in about 20 percent of all patients, and physicians cannot readily predict which patients will benefit before treatment. As such, some physicians choose not to use chemotherapy because of the potential side effects (lung scarring, suppression of the immune system, nausea, etc.).
Chemotherapy works by inflicting cell damage that is better repaired by normal tissue than tumor tissue. Resistance to chemotherapy might involve survival of tumor tissue that cannot respond to the drug, or the inability of the drug to pass from the bloodstream into the brain. A special barrier exists between the bloodstream and the brain tissue called the blood-brain barrier. Some investigators have tried to improve the effect of chemotherapy by disrupting this barrier or by injecting the drug into the tumor or brain. The goal of another class of drugs is not to kill the tumor cells but, rather, to block further tumor growth. In some cases, growth modifiers (such as breast cancer treatment drug Tamoxifen) have been used to attempt to stop the growth of tumors resistant to other treatments.
In 1996, the U.S. Food and Drug Administration approved the use of chemotherapy-impregnated wafers, which can be applied by the neurosurgeon at the time of surgery. The wafers slowly secrete the drug into the tumor, and the patient receives chemotherapy with the systemic side effects of treatment.
Visualase
Laser Thermal Ablation is a newer technique that some centers are using to treat smaller tumors particularly in areas that may be more difficult to reach using previous open surgery procedures. This involves placing a tiny catheter within the lesion, possibly completing a biopsy, then using laser to thermally ablate the lesion. This technique is only more recently used in brain tumor treatments, therefore the long term efficacy has not been established.
Investigational Therapies
Many types of new therapies currently are being studied, especially on tumors for which the prognosis is generally poor through existing conventional therapies. It is unknown whether these therapies will work. Such therapies are given according to a protocol and include various forms of immunotherapy, therapy using targeted toxins, anti-angiogenesis therapy, gene therapy and differentiation therapy. Combinations of treatments also may be able to improve the outlook for patients, while lowering the adverse side effects.
The AANS does not endorse any treatments, procedures, products or physicians referenced in these patient fact sheets. This information is provided as an educational service and is not intended to serve as medical advice. Anyone seeking specific neurosurgical advice or assistance should consult his or her neurosurgeon, or locate one in your area through the AANS’ Find a Board-certified Neurosurgeon”online tool.
Reference: Brain Tumors | American Association of Neurological Surgeons | www.aans.org/Patients